

An Uptick in the Diagnosis of "May-Thurner Syndrome?"
An Uptick in the Diagnosis of "May-Thurner Syndrome?"
The current default-diagnosis of nano-tech blood clotting among the COVID jabbed.

In just the last week, I’ve heard of two individuals who have received the diagnosis of May-Thurner Syndrome. Both are women. Both are jabbed with the COVID bio-weapon shot, and admittedly so, and both are relatively young. One was congresswoman Lauren Boebert and the other was a college student in Virginia, whose professor told me about it from an email the students mother was sending to her professors.
Syndromes don’t occur unless there is a cause. This is where the “S” comes from in the acronym AIDS and VAIDS. The “S” stands for syndrome(s) (i.e., numerous conditions brought about by having a compromised immune system, everything from A to Z).
Blood clots are not hereditary, as we have commonly been told over the years. They’re a direct result from something being introduced into our bodies that damages our DNA. When our DNA is damaged or disrupted, our bodies do not function the way God intended. Therefore, what is the real cause of this condition and is there an uptick in this diagnosis as of late, specifically among the COVID jabbed? Answer: Yes.

Again, something specific causes these syndromes, and doctors tend to not focus on a medical, chemical or habitual cause. Rather, they falsely focus on a series of circumstances that may help the patient and themselves as the doctor, justify the situation. For example, with May-Thurner Syndrome, doctors are quick to answer the question from the patient as to “why has this occurred,” by asking, “are you female, have you given birth, do you exercise with regularity” (even though either a “yes” or “no” answer will still be the excuse to that question) and they may even blame hereditary circumstances. However, none of these are accurate.
Blood clotting, via nanotechnology from the COVID bio-weapon is the only cause, certainly as of late. If blood clotting occurs among men, they don’t call it May-Thurner Syndrome. They just call it blood clotting or Deep Vein Thrombosis (DVT) and they chalk the reason up to something equally as idiotic, like “stress.”
Again, doctors are not trained to look for causes to poor health. They are typically trained to diagnose a condition with a made-up categorized name in a medical book, and then blame some uncontrollable circumstance as to why the patient is in that situation, as if to say (the majority of the time); “There is nothing you could have done. This just sometimes happens.” Then, they prescribe a drug or a procedure in an attempt to cure what ails the person. Unfortunately, with the COVID jabbed and the nano-tech clotting that is occurring, you can’t reverse damaged DNA or turn off a compromised immune system. The DNA will remain permanently damaged and the compromised immune system that results, will continuously attack the body, no matter the drugs they take or the surgical procedures they receive.
This is COVID bio-weapon related. Period.
My only suggestion here, is that you pay attention to those you know who are jabbed and those you hear about, and how many of them are being diagnosed with May-Thurner Syndrome, in particular if they are female.
Any uptick in this diagnosis from a doctor’s perspective will show you that they’ve learned nothing and that they’re simply relying on their emails and medical books to find a reason for their patients current blood clotting. My guess is, doctors everywhere are receiving daily emails about the upticks among patients nationwide who have May-Thurner Syndrome, and they’re being told talking points as to why this is the case and how to “treat” the condition, rather than point the finger at the actual cause; the COVID bio-weapon shots.
Point being, endless doctors haven’t learned anything over the last four years. They’re still relying on the same wavelength of thought that got them here in the first place. Again, pay attention to hearing about this condition more often in the future, as it will most likely be the default diagnosis among the jabbed who are clotting, yet the jabs won’t be named as the reason. Certainly not by their doctors or the hospitals.
To read more about the blood clotting, I recommend Dr. Ana Maria Mihalcea’s Substack above, and the endless documentaries that describe the blood clotting, including Died Suddenly.
However, continue reading below and you will see the symptoms and the circumstances of this “syndrome,” in particular it’s correlation with the COVID bio-weapon shots from a recent peer-reviewed article, published in March of 2024.
First, from Wikipedia:
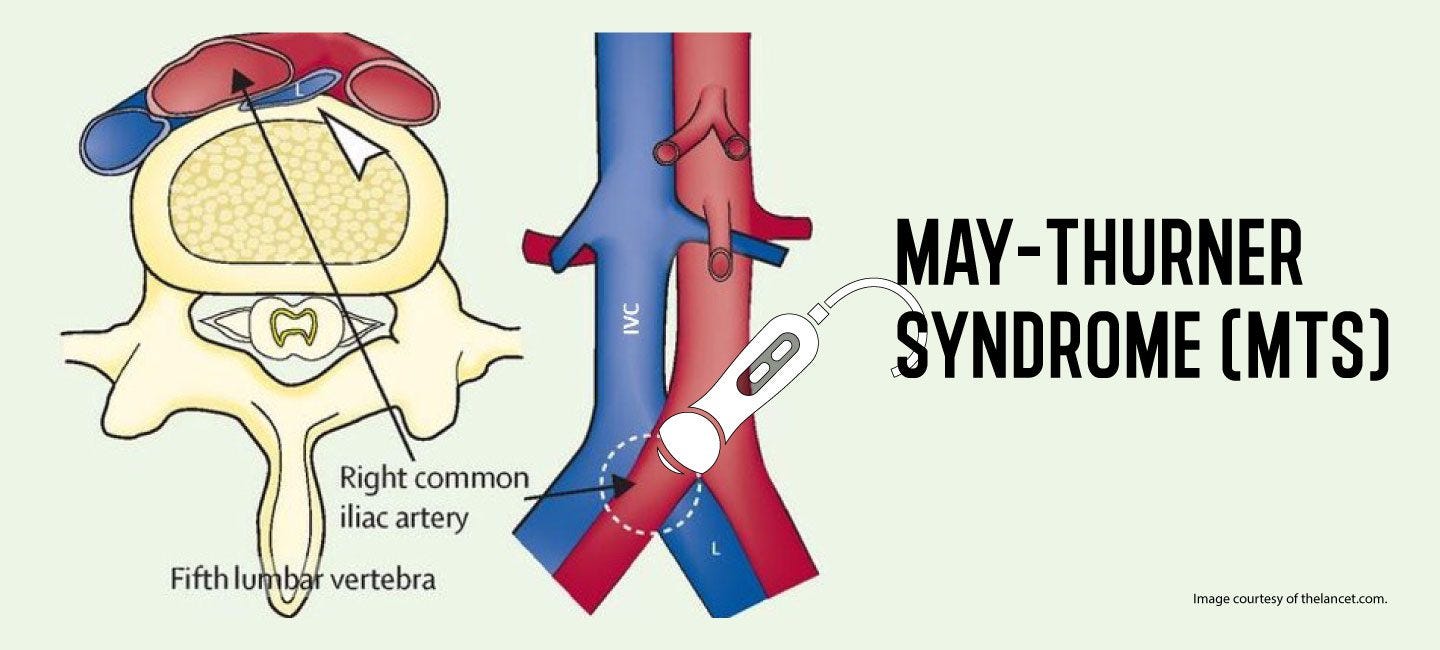
May–Thurner syndrome (MTS), also known as the iliac vein compression syndrome, is a condition in which compression of the common venous outflow tract of the left lower extremity may cause discomfort, swelling, pain or iliofemoral deep vein thrombosis.
Specifically, the problem is due to left common iliac vein compression by the overlying right common iliac artery. This leads to stasis of blood, which predisposes to the formation of blood clots. Uncommon variations of MTS have been described, such as the right common iliac vein getting compressed by the right common iliac artery.
In the 21st century, the May–Thurner syndrome definition has been expanded to a broader disease profile known as nonthrombotic iliac vein lesions (NIVL) which can involve both the right and left iliac veins as well as multiple other named venous segments. This syndrome frequently manifests as pain when the limb is dependent (hanging down the edge of a bed/chair) and/or significant swelling of the whole limb.
Some people with May-Thurner syndrome have no symptoms, but over time, this condition can lead to:
Leg swelling.
Chronic venous insufficiency, in which blood pools in your veins. This causes swelling, pressure, skin changes, and venous ulcers or sores that don't heal.
Deep vein thrombosis (DVT), a blood clot in a vein deep below your skin.
If a blood clot breaks free and travels to your lungs, heart, or brain, it can lead to serious, even life-threatening issues like:Pulmonary embolism, a blood clot in your lung
Below is the abstract from a review article on the subject of May-Thurner Syndrome. It stated the following:
Abstract: May-Thurner syndrome is a rarely diagnosed condition in which patients develop iliofemoral deep venous thrombosis (DVT) due to an anatomical variant in which the right common iliac artery overlies and compresses the left common iliac vein against the lumbar spine. This variant has been shown to be present in over 20% of the population; however, it is rarely considered in the differential diagnosis of DVT, particularly in patients with other risk factors. Systemic anticoagulation alone is insufficient treatment, and a more aggressive approach is necessary to prevent recurrent DVT. Herein, we present a patient with multiple risk factors for DVT. With a comprehensive diagnostic approach, she was found to have May-Thurner syndrome. Local infusion of thrombolytics as well as mechanical thrombectomy failed to resolve the thrombus. Subsequently the patient underwent successful stent placement in the area that was compressed followed by 6 months of chronic anticoagulation with warfarin. There has been no recurrence of DVT in the ensuing 18 months.
The long term prognosis and complications from May-Thurner Syndrome (i.e., blood clotting) are outlined in the article above of the same name, and listed below. They stated:
A few pearls regarding May-Thurner syndrome:
Although MTS accounts for only 2% to 5% of all patients presenting with DVT, multiple autopsy studies have shown that the actual prevalence is as high as 14% to 32% in the general population.
Despite the high prevalence, MTS remains clinically silent in most patients.
Iliofemoral DVT is the most common presentation of MTS.
Young women are at a higher risk of developing DVT compared to men.
A transient risk factor is usually present in patients with MTS, which precipitates the thrombotic event.
MTS has been associated with patent foramen ovale and cryptogenic stroke.
Prompt anticoagulation with low-molecular-weight heparin or fondaparinux is needed to prevent PE.
Although most societies recommend warfarin for long-term anticoagulation, recent studies show that rivaroxaban is equally effective and has a lower risk of major bleeding (although this has not reached statistical significance in clinical studies).
Venogram with IVUS is the gold standard in diagnosing MTS. In addition to diagnosis, it also helps in the treatment of DVT secondary to MTS.
Catheter-directed thrombolysis, followed by stent placement, is the treatment of choice.
Surgical resection of thrombus is falling out of favor. It is reserved for patients in whom endovascular treatment fails.
Anticoagulation alone is not sufficient to treat patients with DVT secondary to MTS. It should be combined with catheter-directed thrombolysis.
Post-thrombotic syndrome is the most common adverse event after developing iliofemoral DVT. Residual thrombus after thrombolysis and stent placement is positively associated with the risk of developing PTS.
A recent article titled; Post-COVID-19 Vaccine Thromboembolic Complication in the Setting of Newly Diagnosed May-Thurner Syndrome, described the correlation between the COVID shots and May-Thurner syndrome. It was published in March of 2024. The abstract states the following:
Abstract: May-Thurner syndrome (MTS) can lead to deep venous thrombosis (DVT) in the left lower extremity, and it is often triggered by factors such as surgery or pregnancy. We present a rare case where the risk factor for thromboembolism in MTS is a complication from COVID-19 vaccination. A 44-year-old female who presented with fatigue, fever, and myalgia had developed thromboembolism as a complication of the Johnson & Johnson COVID-19 vaccine. Diagnostic criteria for vaccine-induced immune thrombotic thrombocytopenia (VITT) should be considered in such cases that include symptoms within 5-30 days post vaccination, elevated D-dimer, and thrombosis. Treatment involved anticoagulants and intervention for MTS included thrombectomy and stent placement. Recognition of post-COVID-19 vaccination complications such as VITT is crucial for early intervention and patient awareness during vaccination decisions.
These will be reoccurring conditions among the jabbed. There is no “cure” for this. There is only a short-term possible remedy, but there is no reversal from what the COVID jabs have done. If the diagnosis of May-Thurner syndrome (MTS) becomes overused in the near future, doctors will simply switch names or syndromes in place of May-Thurner syndrome (MTS), as there are endless syndromes that are related to and identified by blood clotting.
Case in point, Deion Sanders.

Deion Sanders, the coach of the University of Colorado’s football team, is COVID jabbed and has continuous blood clotting throughout his legs and in one of his hips. He’s had toes amputated, parts of one of his legs removed (picture above, look at his inner calf), arteries and veins re-routed on his lower extremities and his DNA is forever ruined and his compromised immune system is not turning off. This will continue until Deion Sanders is dead.
I’m certain Deion Sanders, his doctors, nor those around him are not striking up his ailment to the COVID bio-weapon. They’re most likely blaming his race, family history, football injuries, or even his past athleticism; if not his age. All of these are lies. The only cause of this, and its continuous negative progression, is damaged DNA and a compromised immune system from the COVID bio-weapon. Yet, he and those around him have no clue.
There are endless people like him in the limelight who are injured from the COVID bio-weapon and endless more who are not in the limelight. Yet, they all have one thing in common.
Again, with the COVID jabbed and the nano-tech clotting that is occurring, you can’t reverse damaged DNA or turn off a compromised immune system. The DNA will remain permanently damaged and the compromised immune system that results will continuously attack the body, no matter the drugs they take or the surgical procedures they receive.
BIO: Dr. Sean M. Brooks is the host of the podcast American Education FM and the author of several books including; The Unmasking of American Schools: The Sanctioned Abuse of Americas Teachers and Students. He’s also on Gab, Truth, X, Bitchute, Rumble and everywhere audio podcasts can be heard.
Some say nattokinase might be useful with this isht. Others, I've heard, try to combine that with detox and a few days' fast. People are inventive and our bodies absolutely rock when given the chance.
I'm a new reader, just stumbled on your substack yesterday and been catching up. Interesting stuff, hat lift, sir. It's sickening what's been done with these shots, but I wouldn't want to add to the distress someone who's taken the jab(s) and later come to their senses must be feeling, not if there's some hope left, or maybe to be found tomorrow. Let's try to add hope when little is left.
Cheers.
Colleague from Santaland
Not about the topics in this article, but please check this out: https://www.bitchute.com/video/1hbdRxBBKmAg/