Political infiltration, corruption, whistleblowing, crime, history, health, philosophy, experiences, medical tyranny, and the collapse of American K12 and university education.
First of all, Substack is telling me this article is too long for email. My recommendation is that you go over to my actual Substack page, The American Classroom, and check this one out. My apologies for the length of this one, but I have numerous points to make here.
With that said, I’ve covered these subjects in the past on my podcast audio show, American Education FM. If you follow me here on Substack, I recommend giving that show a listen if you haven’t in the past. I cover way more information there, than I can here on Substack in an article. However, this subject deserves a re-visit and then a suggestion for a new trend that would be an enjoyable one to see at school-board meetings (just for the reaction). I’ll get to that later in the article.
Just to review, we know that Americans schools are degenerate, failing, and supporting the most Marxist and communistic agendas which align with Satan himself. After all, it the Marxist and communistic agendas that were created by satanic jews and those who worship satan, so the leap is not a far one to make. But, with that said, allow me to revisit a common issue regarding the LGBTQ satanic agenda and what these schools are really supporting when they advocate for mentally ill students, their mentally ill parents, and the final result of this mental illness.
American schools claim to always advocate for the end result. For example, they claim to have all of their students “academically succeed” so that they’re “successful later in life.” Sadly, they’re also advocating for the untimely death of students whether they know it or not.
Case in point, the school-board members of the Westerville City School District in Westerville, Ohio. Back in January of 2024, they published a statement supporting all LGBTQ+ students and staff, while openly and collectively opposing the Ohio House of Representatives overturning of Governor Mike DeWine’s veto of HB 68. This bill, which is now law (thank God), outlaws hormone blockers, sex-reassignment surgery, genital mutilation, transgender bathrooms of choice, and it bars transgender wack-jobs from playing in a sport of their choice, in particular playing a sport against the opposite biological sex.
In response to the overridden veto and newly pronounced law, the Westerville City School District in Westerville, Ohio made the following public response, as they again, openly support the less than 1% at the expense of the other 99%:
-Jan 26 2024:
“Where You Belong” is more than a slogan in Westerville City Schools. It’s a guiding principle that reminds us of our obligation as a public school system to provide environments in which everyone feels safe, valued, respected, and included.
Ohio’s 135th General Assembly recently acted to override the Governor’s veto of House Bill 68 which, among other things, prevents transgender athletes from playing women’s sports. Legislating such discriminatory measures against Ohio’s LGBTQ+ community now makes it impossible for educational leaders across the state to create educational environments and provide opportunities for ALL children.
HB68 will take effect towards the end of April. While we have no choice but to comply with the law, no child should feel discriminated against or marginalized. To that end, we will strive to ensure other established supports remain in place for the LGTBQ+ children in our schools. Please know that despite any present and future roadblocks implemented by State leaders, the Westerville City School District remains committed to providing educational experiences and environments that support ALL students – especially if they are part of an already-vulnerable group of children.
Our school counselors are available to speak with any students who may need additional support during this challenging time. As an institution, we work hard to recognize, honor, and celebrate the diversity found in our community and our schools. We remain steadfast in our efforts to ensure that children learn in safe environments that are welcoming and inclusive for EVERYONE. And, we would like our transgender students and their families to know that you are loved, you are supported, and the Westerville City School District will always be a place Where You Belong.”
This is just one school district which exists in an Ohio town that is made up of mainly conservative to independent voters. Frankly, politics at this point are irrelevant, as even many within those two voting groups are dead asleep as to what is going on in the real world. With that said, however, this is a school district that has just doubled-down on the final result of supporting the LGBTQ satanic agenda.
The reason I say they’re supporting the “final result,” is that you can’t support those who have gender dysphoria (which is a categorized mental disorder) and not support what they do to themselves and the final result that comes with it, which includes, but is not limited to; gender reassignment surgery, drug addiction, sexual promiscuity, abortion, violence, advancing mental illness, failing to get the mentally ill help, murder, suicide, and normalizing all of the variables that lead to these actions.
While some continue to attend school-board meetings and read from pornographic books that exist within their libraries (in an effort to confront the sexual perverse school-board members and their policies), how about we kick it up a notch?
Before pulling your children out of American schools forever, how about showing up at a school-board meeting and describing “gender-affirming surgery” and the elements I’ve listed above that are the middle-to-end result of what they’re actually supporting when they wave the rainbow flag and support the LGBTQ agenda? Given that over 75% of all humans are visual learners, how about we give them a show? Why not show them what they actually advocate for? Why not make posters of the following pictures and make them face their own reality?
Phalloplasty among Gender Dysphoria individuals:
Final result of a Phalloplasty procedure (above).
Phalloplasty procedure using the grafted skin from the forearm to wrap around a plastic phallic device with a catheter inserted within (above).
The following written description comes from an article titled “Female-to-male gender-reassignment surgery:”
“A person may wish to undergo this type of surgery if they are uncomfortable having a uterus, ovaries, or fallopian tubes or if hormone therapy does not stop menstruation. In a partial hysterectomy, a surgeon will remove only the uterus. In a total hysterectomy, they will also remove the cervix. A bilateral salpingo-oophorectomy involves the removal of the right and left fallopian tubes and ovaries.
A metoidioplasty is a method of constructing a new penis, or neopenis. Research from 2021 shows this procedure has a low risk of complication and a high satisfaction level. A metoidioplasty has positive cosmetic and functional outcomes. This procedure involves changing the clitoris into a penis. A person will receive hormone therapy before the surgery to enlarge the clitoris for this purpose. During the procedure, the surgeon also removes the vagina in a vaginectomy. In addition, they lengthen the urethra and position it through the neopenis. To achieve the lengthening, the surgeon uses tissues from the cheek, labia minora, or other parts of the vagina. The aim of this is to allow the person to urinate while standing. An advantage of metoidioplasty is that the neopenis may become erect due to the erectile abilities of clitoral tissue.
A phalloplasty uses grafted skin (above) — usually from the arm, thigh, back, or abdomen — to form a neopenis. Compared with a metoidioplasty, a phalloplasty results in a larger penis. However, this neopenis cannot become erect on its own. After a period of recovery, a person can have a penile implant. This can allow them to get and maintain erections and have penetrative sex. Disadvantages of a phalloplasty include the number of surgical visits and revisions that may be necessary, as well as the cost, which is typically higher than that of a metoidioplasty.
A person may decide to have a scrotoplasty — creating a scrotum — alongside a metoidioplasty or phalloplasty. In a scrotoplasty, a surgeon hollows out and repositions the labia majora to form a scrotum and inserts silicone testicular implants.
The recovery time from female-to-male surgery varies, depending on the type of procedure and factors such as the person’s overall health and lifestyle choices. For example, smoking slows down recovery and increases the risk of complications following surgery. Following gender-affirming surgery, most people need to stay in the hospital for at least a couple of days. After leaving the hospital, the person must rest and limit strenuous activity.
As with any surgery, all gender-affirming surgeries carry a risk of:
-infection
-bleeding
-reactions to anesthesia
Some complications of a metoidioplasty or phalloplasty include:
-Urethral fistula: A tunneled connection that forms between the urethra and another part of the body.
-Urethral stricture: A narrowing that causes a blockage of urine flow within the urethra.
A person who has had a phalloplasty may experience scarring in the area where the surgeon has taken the graft or a skin graft failure.”
Vaginoplasty procedure among Gender Dysphoria individuals:
End result after Vaginoplasty surgery: https://www.frontiersin.org/articles/10.3389/fsurg.2021.639430/full
The following description of vaginoplasty surgery and the pictures of the procedure itself, come from Frontiersin.org:
At our institution, we perform the classic penile inversion vaginoplasty, with an inverted penis skin flap used as the lining for the neo-vagina. For more details, we have previously published our technique with a step-by-step procedure video (6).
All individuals underwent intestinal cleansing the evening before the surgery. A first-generation cephalosporin was used as preoperative prophylaxis. The procedure was performed with the patient in a dorsal lithotomy position. A Foley catheter was placed for bladder catheterization. A inverted-V incision was made 4 cm above the anus and a flap was created. A neovaginal cavity was created between the prostate and the rectum with blunt dissection, in the Denonvilliers space, until the peritoneal fold, usually measuring 12 cm in extension and 6 cm in width. The incision was then extended vertically to expose the testicles and the spermatic cords, which were removed at the level of the external inguinal rings. A circumferential subcoronal incision was made (Figure 1), the penis was de-gloved and a skin flap was created, with the de-gloved penis being passed through the scrotal opening (Figure 2). The dorsal part of the glans and its neurovascular bundle were bluntly dissected away from the penile shaft (Figure 3) as well as the urethra, which included a portion of the bulbospongious muscle (Figure 4). The corpora cavernosa was excised up to their attachments at the symphysis pubis and ligated. The neoclitoris was shaped and positioned in the midline at the level of the symphysis pubis and sutured using interrupted 5-0 absorbable suture. The corpus spongiosum was reduced and the urethra was shortened, spatulated, and placed 1 cm below the neoclitoris in the midline and sutured using interrupted 4-0 absorbable suture. The penile skin flap was inverted and pulled into the neovaginal cavity to become its walls (Figure 5). The excess of skin was then removed, and the subcutaneous tissue and the skin were closed using continuous 3-0 non-absorbable suture (Figure 6). A neo mons pubis was created using a 0 absorbable suture between the skin and the pubic bone. The skin flap was fixed to the pubic bone using a 0 absorbable suture. A gauze impregnated with Vaseline and antibiotic ointment was left inside the neovagina, and a customized compressive bandage was applied (Figure 7 shows the final appearance after the completion of the procedures).
Postoperative Care and Follow-Up
The patients were usually discharged within 2 days after surgery with the Foley catheter and vaginal gauze packing in place, which were removed after 7 days in an ambulatorial attendance.
Our vaginal dilation protocol starts seven days after surgery: a kit of 6 silicone dilators with progressive diameter (1.1–4 cm) and length (6.5–14.5 cm) is used; dilation is done progressively from the smallest dilator; each size should be kept in place for 5 min until the largest possible size, which is kept for 3 h during the day and during the night (sleep), if possible. The process is performed daily for the first 3 months and continued until the patient has regular sexual intercourse.
The follow-up visits were performed 7 days, 1, 2, 3, 6, and 12 months after surgery (Figure 8), and included physical examination and a quality-of-life questionnaire.
If the above information and pictures are disturbing to you, good. They should be. That’s the point, because the truth is disturbing. This is exactly what American schools are supporting daily, yet it’s the supporters themselves who are blatantly hypocritical in their rhetoric. If presented with these facts and images, they will admonish the message and the messenger, turn away, end the conversation/presentation by adjourning, and then sit with their own lack of knowledge or rationalized dismissal of the real subject at hand; that it’s they themselves who openly support the final result without ever wanting to see it, hear about it or learn about it.
Ask yourself this: do people build a house for themselves without living in it? Do they buy a car and then not drive it? Does an artist paint a paining without looking at it, or does an art gallery hang such art work without observing it once it’s hanging? If not, then why would it be so hard for American school officials to view the final result of what they advocate for in the first place? Simple. They’re demonic, brainwashed hypocrites, and parents still send their children to these environments. Yet, if a babysitter advocated for this demonic behavior, parents would never send their children to said babysitter.
See the effectiveness of brainwashing? See the hypocrisy?
You also, of course, have to accept the short and long term ramifications of acquiring and owning the acceptance of such material objects. For example, with the owning of a house, one may need a new roof. With the owning of a car, one may need new tires if they become flat. Or, as with an artist, you’ll have to receive the criticism that may come from people not liking your art. Yet, it’s these realities that schools fail to accept, nor take responsibility for when they advocate for the satanic LGBTQ agenda and ultimately the final result of that advocacy.
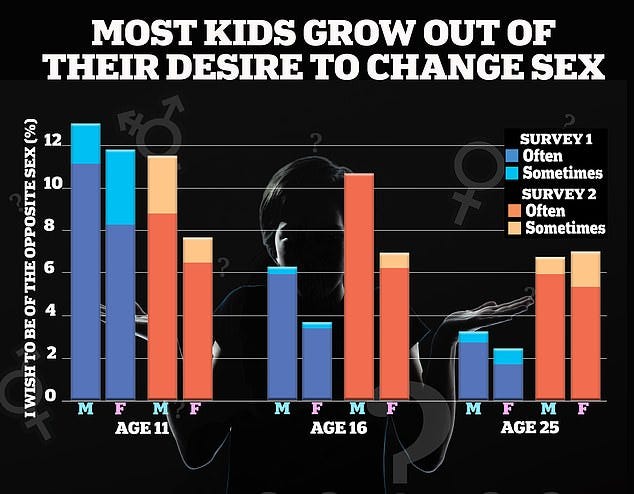
Unfortunately, the war on information is an on-going war, too. So much so, that the once advocates of this jewish-satanic movement are now claiming that most “gender confusion” is “outgrown” in time. This, unfortunately, is another myopic dismissal of the short and long-term life-altering consequences of this kind of advocacy.
You see, there was a time when playing with GI-JOES or stuffed animals was a childhood activity that was out-grown with aging. But, cutting your dick off or having a fake one sewn on your vagina—is a permanent activity with permanent consequences, that can lead to one’s suicide and untimely death.
‘Indeed, we can infer from the DSM 5 [2013] and other sources that as many as 88 percent of gender-dysphoric girls and as many as 98 percent of gender-dysphoric boys in previous generations desisted if allowed to go through natural puberty.
'These two facts make it clear why “gender-affirming care” on minors is such an outrage. It leads, in the end, to sterilization and in many cases to a complete loss of natural sexual function.
'There is no good evidence that this helps minors long term. Moreover, it medicalizes what could very well be temporary psychological symptoms.
'History will judge this medicalized “gender-affirming care” on minors as we now judge eugenics and lobotomies.’
(The research was published in theJournal Archives of Sexual Behavior).
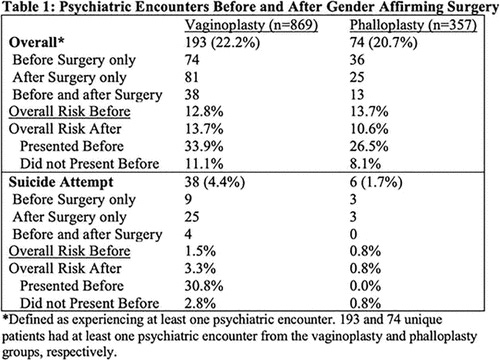
“Results: Overall, 869 and 357 patients were identified undergoing vaginoplasty and phalloplasty with 193 (22.2%) and 74 (20.7%) having at least one psychiatric encounter (Table 1). Although the overall proportion of those experiencing a psychiatric encounter was similar between the vaginoplasty and phalloplasty groups, suicide attempts were more common in the vaginoplasty group (4.4% vs. 1.7%, p=0.033). The rate of a psychiatric encounter occurring after surgery if an episode prior surgery occurred was 33.9% and 26.5% for the vaginoplasty and phalloplasty groups. The overall rates of suicide attempts doubled (3.3 vs 1.5%, p=0.017) after vaginoplasty (effect not observed after phalloplasty).”
“Conclusions: Rates of psychiatric emergencies are high both before and after gender affirming surgery. Although both the phalloplasty and vaginoplasty patients have similar overall rates of psychiatric encounters, suicide attempts are more common in the later. In fact, our observed rate of suicide attempts in the phalloplasty group is actually similar to the general population, while the vaginoplasty group's rate is more than double that of the general population. Patients undergoing GAS with a history of prior psychiatric emergences or feminizing transition are at higher risk and should be counseled appropriately.”
It must also be stated that the advancement of homosexual behavior within schools, in particular its normalization among youth, can also be a precursor to the final result. This, too, is being pushed without thought of the final result among those who lead American schools. They, too, are not interested in really hearing the facts of what they’re actually advocating for, so let’s remind them.
58% OF HOMOSEXUALS HAVE PROBLEMS WITH INTESTINAL WORMS.
1 IN 15 HOMOSEXUALS IS A PEDOPHILE.
33% OF HOMOSEXUALS HAVE PROBLEMS WITH ALCOHOLISM.
PERFECT CORRELATION BETWEEN CHILDHOOD RAPE AND HOMOSEXUAL BEHAVIOR.
47% OF GAYS ADMIT TO HAVING BEEN RAPED BY AN ADULT MAN DURING THEIR CHILDHOOD OR ADOLESCENCE.
78% OF HOMOSEXUALS HAVE STDS (SEXUALLY TRANSMITTED DISEASES).
HOMOSEXUALS REPRESENT 2% OF THE WORLD'S POPULATION BUT THEY REPRESENT 67% OF AIDS PATIENTS (https://archive.ph/scA5b).
ON AVERAGE, A GAY MAN HAS UP TO 80 SEXUAL PARTNERS PER YEAR AND ON AVERAGE A TOTAL OF 1,000 OVER A LIFETIME.
ON AVERAGE, A STRAIGHT MAN HAS 8 SEXUAL PARTNERS IN HIS LIFETIME.
HOMOSEXUALS REPRESENT 2% OF THE WORLD'S POPULATION BUT THEY REPRESENT 33% OF PEDOPHILE RAPISTS (https://archive.ph/sX8zg).
23% OF CHILDREN WITH LESBIAN PARENTS HAVE BEEN SEXUALLY ABUSED (https://archive.ph/5UPbM).
51% OF CASES OF DOMESTIC VIOLENCE OCCUR IN SAME-SEX COUPLES.
(Note the sourced websites to the statistics in the meme above).
Schools also dare not read the history involved in the very movements they advocate for, because they actually think that these movements are natural and pop-up out of thin air. You’ll never catch school-board members, nor teachers or administrators, learning about the monsters who created these movements, performed these mutilations as a profession, nor will school employees ever say their names. The likes of Magnus Hirschfeld and Stanley Biber are not likely to be the subjects of a book report, nor a history-fair project among the student population, but perhaps it’s time they are.
Magnus Hirschfeld himself, has one of the largest Wikipedia pages I’ve ever seen and he was a homo-jewish monster of the highest order. Thank God Adolf Hitler shut down Hirschfeld’s operation and work. He should have shot him. Oh, and Hirschfeld’s books were among those that the German citizens famously burned. Looks like Adolf was right again.
Ladies and gentlemen, American schools advocate for all of the above. So does Satan. Just look at the grip that the jewish lobby has on the entire business. Do you actually think this can be “reformed?” Do you actually think this can be reversed?
So, how about you kick it up a notch? Instead of reading from pornographic books and still sending your children back to the same schools that offer them in their libraries (and they ALL DO), how about you show these schools and the jewish lobbies that control them, the final result of what they’re really supporting?
American schools and their employees aren’t supporting real mental health nor any real therapy for minors who attend either. These environments are the cause of the mental illness and they don’t even know it, so it’s impossible that they would be the saviors of it. Schools also aren’t helping the mental illness that is prevalent among the parents themselves who support their children who are pretending to be a sex of which they are not, while also advocating for all of the above. Frankly, it’s not even their job. A school board or any other school employee’s entire belief of their own job description has been warped, permanently.
American schools are only advocating for the final result of such mental illness. That final result of mental illness, is always death.
Therefore, stop supporting American schools, advocate for home-learning and home-schooling, and lead by example with the removal of your own children from American schools—now and forever.
This is obscene. Just scanning through those photographs, this is absolutely obscene. I'm supposed to believe that "Transgenderism" is acceptable when this article proves it's the most atrocious psychosis imaginable? But up here in Justine Castreau's Woke Democratic Socialist Non-White People's Republic of Canuckistan? Just to repost this, I'm risking a visit from "The Social Justice Tribunals" and a $250,000 fine plus paying the plaintiff's costs.
And when – not if – they pass their "On-Line Harms Act", I could be facing life imprisonment, for posting Hate Speech.
I forced myself to read this entire post…even as my eyes welled up. Holy f*%ck. It’s also not the first time I have seen photographed results of these surgeries. It literally just doesn’t get any easier for my eyes to see, each time they do.

















This is obscene. Just scanning through those photographs, this is absolutely obscene. I'm supposed to believe that "Transgenderism" is acceptable when this article proves it's the most atrocious psychosis imaginable? But up here in Justine Castreau's Woke Democratic Socialist Non-White People's Republic of Canuckistan? Just to repost this, I'm risking a visit from "The Social Justice Tribunals" and a $250,000 fine plus paying the plaintiff's costs.
And when – not if – they pass their "On-Line Harms Act", I could be facing life imprisonment, for posting Hate Speech.
https://www.youtube.com/watch?v=y4-L0-s6llU
I forced myself to read this entire post…even as my eyes welled up. Holy f*%ck. It’s also not the first time I have seen photographed results of these surgeries. It literally just doesn’t get any easier for my eyes to see, each time they do.